
By Rebeca Segraves, PT, DPT
A woman lies in a hospital bed at Intermountain Medical Center, exhausted after her fifth cesarean section. In less than a decade, she has been through five major abdominal surgeries. Yet this time, something startling happens. For the first time, someone shows her how to do a bridge. For the first time, someone teaches her how to breathe in a way that supports her core. For the first time, someone explains how an abdominal binder can help stabilize her incision when she gets out of bed to care for her baby.
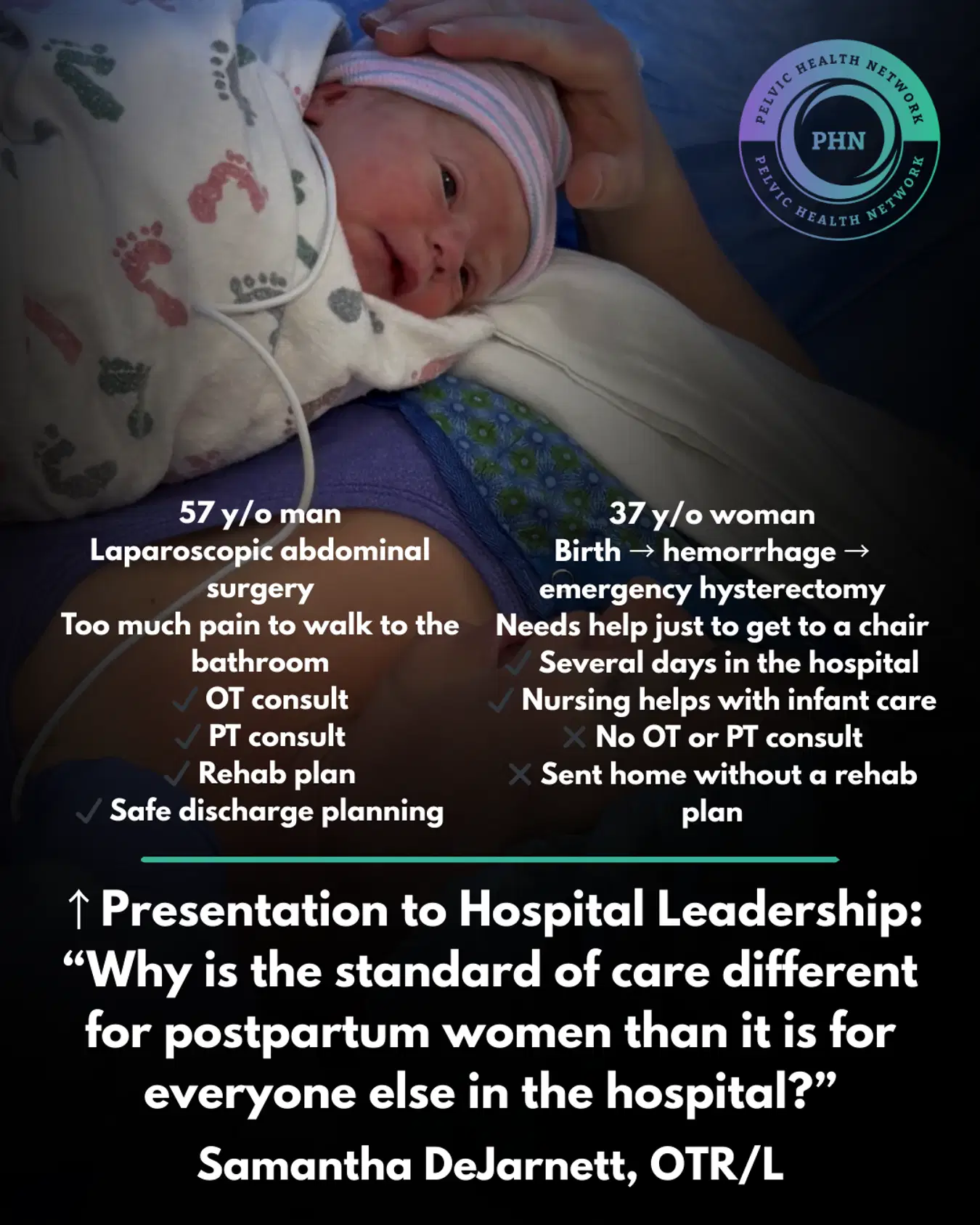
That moment, simple on its face, says something unsettling about postpartum care in the United States. A patient can go through five C-sections before anyone treats her recovery like surgical recovery.
For years, hospitals have accepted a strange double standard. If a patient has a knee replacement, therapy often begins the same day. If a patient has a cardiac procedure, mobility starts early and deliberately. But if a mother has a C-section, the most common major surgery in the country, she is often discharged with a newborn, a fresh incision, and little more than a six-week follow-up appointment on the calendar.
That six-week wait has long been framed as routine. In practice, it can look more like abandonment.

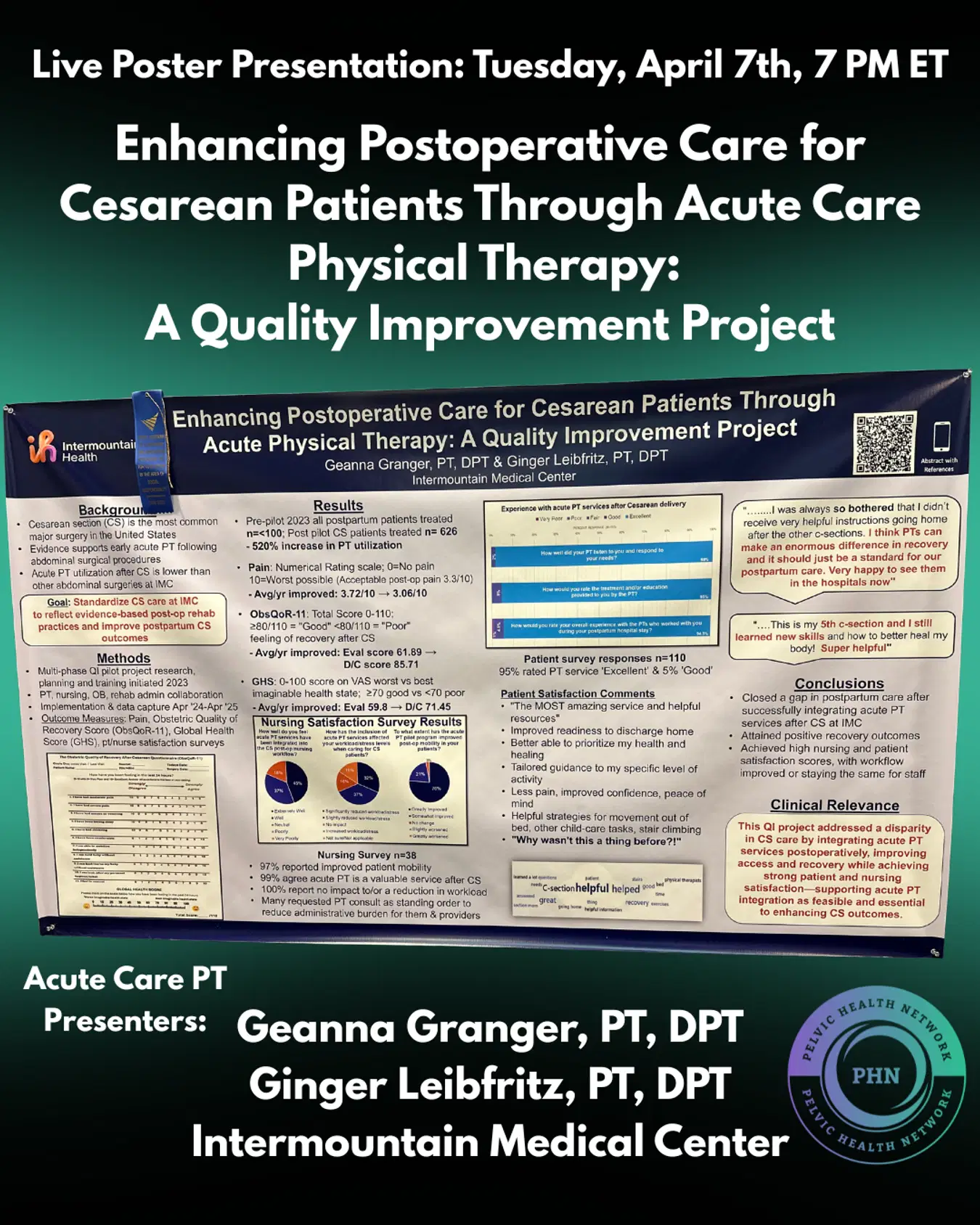
At Intermountain Medical Center, two physical therapists, Geanna Granger, PT, DPT, and Ginger Leibfritz, PT, DPT, decided to question that routine. Their quality improvement project did not begin with a sweeping policy change or a national campaign. It began on the maternity floor, with a practical idea: what if mothers recovering from C-sections received the same early rehabilitation mindset that hospitals already accept in other areas of medicine?
The need was not subtle. Cesarean deliveries account for about 32% of births in the United States, more than 1.1 million procedures each year. Even so, postpartum recovery has remained oddly underbuilt. Mothers are expected to manage pain, mobility, lifting, infant care, and basic function with minimal instruction. While patients undergoing orthopedic procedures like knee or hip replacements receive immediate, structured physical therapy, postpartum mothers are often left to navigate their recovery without any professional guidance on lifting or basic mobility.
Granger and Leibfritz built their pilot to disrupt that pattern. They standardized physical therapy involvement for C-section patients and measured what happened next. The results were difficult to ignore. Before the project, the maternity unit had fewer than 100 physical therapy orders in a year. After the new workflow took hold, orders increased by 520%.
“We were not uncovering a small, niche need,” Granger said, reflecting the team’s findings. “We were exposing how much care had been missing in plain sight.”
The intervention itself was not flashy. Therapists helped patients move safely in and out of bed. They taught breathing strategies, incision support, lifting mechanics, and binder use. They addressed pelvic floor concerns and early function. In other words, they treated postpartum recovery as recovery.
To track outcomes, the team used the Obstetric Quality-of-Recovery score, or ObsQoR-11, a validated measure that captures how well a patient can mobilize, care for herself, and function after delivery. Many patients started below the threshold associated with a good recovery. After therapy, scores improved. So did confidence. Patients were leaving the hospital with more than discharge paperwork. They were leaving with skills.
For the woman after her fifth C-section, that difference felt immediate. What had once been presented as something women were simply supposed to endure now looked like a solvable systems problem.
That is part of what makes the data so striking. The project was not centered on rare technology or a high-cost intervention. It was built around basic rehabilitation, delivered early, by clinicians who understood that birth does not cancel out surgery.
The impact reached beyond patients. In many hospitals, new programs face resistance because leaders assume they will add work for already overextended nurses. At Intermountain, the opposite happened. As therapists took on ambulation, binder fitting, and movement education, nurses reported relief, not burden.
Leibfritz described the cultural shift as one of the most important findings in the project. “Once nurses saw that this helped patients and eased pressure on the floor, they stopped seeing therapy as an extra,” she said, reflecting the clinical results. “They became some of the strongest advocates for getting these patients seen early.”
That shift showed up in the patient experience data, too. The unit maintained patient recommendation scores above 90% throughout the year. For a hospital metric that can rise and fall for countless reasons, the consistency mattered.
“You could feel the culture changing,” Granger said, based on the team’s observations. “Nurses were identifying the patients who needed support and asking for orders before rounds. That is when you know a pilot is becoming a new standard.”
What happened on the maternity floor was not just an improvement project. It was a challenge to a deeply embedded assumption in American medicine, the idea that postpartum patients can wait, manage, and figure it out later.

That assumption has consequences. Delayed support can leave mothers struggling with pain, fear of movement, poor lifting mechanics, and limited mobility at the exact moment they are also learning to feed, soothe, and carry a newborn. The burden is clinical, but it is also cultural. Birth is often treated as a natural event, while the surgery, tissue trauma, and physical demands surrounding it fade into the background.
Intermountain’s pilot suggests a different model. The six-week wait does not have to define postpartum care. Early therapy can begin in the hospital. Recovery education can be standardized. Functional outcomes can improve. Nurses can become allies rather than gatekeepers. And patients who once slipped through the cracks can finally be seen.
For families trying to identify hospitals that offer this kind of early rehabilitation, the postpartum recovery hospital directory provides a starting point.
References
Granger G, Leibfritz G. Integrating Acute Care Physical Therapy for Cesarean Patients at Intermountain Medical Center: A Quality Improvement Project. Poster presented at: APTA Combined Sections Meeting; February 2026; Anaheim, CA.
Ciechanowicz S, Howle R, Heppolette C, Nakhjavani B, Carvalho B, Sultan P. Evaluation of the Obstetric Quality-of-Recovery score (ObsQoR-11) following non-elective caesarean delivery. Int J Obstet Anesth. 2019;39:51-59. doi:10.1016/j.ijoa.2019.01.010.
Segraves RL, Croghan A, Coreas M, Locati E, Finley RN. Initiating occupational and physical therapy in the hospital after birth: access, reimbursement, and outcomes. J Womens Pelvic Health Phys Ther. 2023;47(1):15-26. doi:10.1097/JWH.0000000000000262.


